
Before the First Breath: Airway Inflammation as a Driver of Placental and Fetal Immune Programming
A Clinical Perspective in Systems Biology
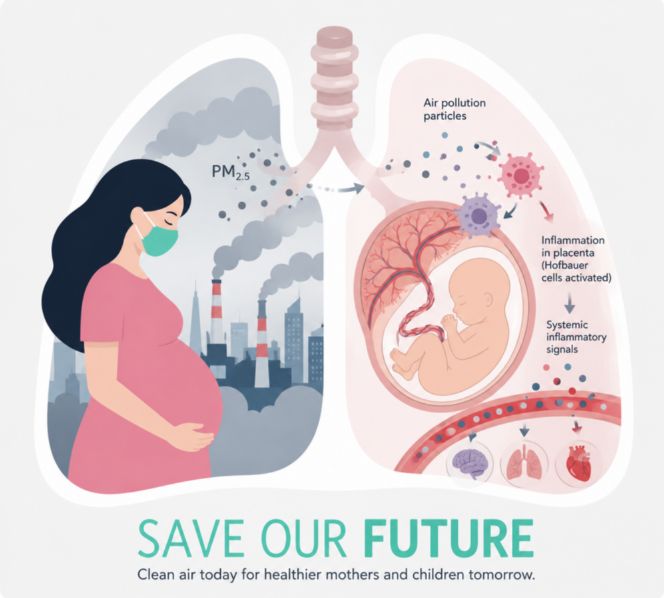
Emerging evidence suggests that the effects of prenatal air pollution are mediated not only through direct deposition of particulate matter within the placenta, but also through a broader mechanism of maternal airway-driven systemic inflammation. In this framework, the lung serves as the primary environmental sensor, initiating inflammatory signaling that propagates through the circulation and alters placental structure, immune balance, and fetal development. Integrating recent mechanistic insights from placental biology with systems-level inflammatory models provides a more unified understanding of how environmental exposures shape early life and opens new pathways for clinical intervention.
Introduction: Beyond Isolated Organ Models
Air pollution has traditionally been studied in discrete domains such as pulmonary injury, cardiovascular disease, or adverse pregnancy outcomes. Yet these categories are artificial boundaries imposed on what is, biologically, a continuous system.
The placenta shares key features with the airway epithelium. Both are highly vascular, immunologically active, and designed to interface with the external environment, directly or indirectly. Recent work demonstrating rapid disruption of placental microarchitecture following exposure to fine particulate matter challenges the notion that fetal exposure is merely passive. Instead, the placenta emerges as an active participant in a systemic inflammatory network, responding dynamically to environmental stressors.
This perspective suggests that placental injury is not an isolated phenomenon but part of a broader process driven upstream by airway inflammation.
The Lung as the Initiator of Systemic Signaling
The respiratory system represents the largest interface between the human body and the external environment. When fine particulate matter is inhaled, it reaches the distal airways and alveoli, where it activates immune and epithelial cells. This activation leads to the release of inflammatory mediators and the generation of oxidative stress, often in the absence of overt respiratory symptoms.
These early inflammatory changes frequently occur below the threshold of clinical detection. Conventional tools such as pulse oximetry and basic spirometry typically identify only later stages of disease, when gas exchange is already compromised. However, long before that point, the lung may already be functioning as a source of systemic inflammatory signaling.
Once initiated, these signals disseminate through the bloodstream. Cytokines, oxidized molecules, and stress mediators circulate throughout the body, establishing a state of chronic low-grade inflammation that can influence distant organs.
The Placenta as Target and Amplifier
Within this systemic context, the placenta becomes both a target and an amplifier of inflammatory processes.
Direct exposure occurs when particulate matter or its associated compounds enter the circulation and reach placental tissue. Experimental studies demonstrate that particles can embed within placental cells and disrupt structural integrity within minutes. The extracellular matrix, which provides mechanical stability to the villous architecture, begins to degrade rapidly, leading to cellular detachment and tissue instability.
At the same time, the placenta is exposed to circulating inflammatory signals originating in the maternal lungs. This indirect pathway may be equally significant. Cytokines and oxidative stress mediators alter placental function, affecting not only structural components but also endocrine signaling and vascular regulation.
The convergence of these direct and indirect mechanisms creates a dual-hit model in which the placenta reflects and amplifies systemic inflammatory tone.
Hofbauer Cells and Immune Reprogramming
A key mechanistic link between maternal inflammation and fetal development lies in the behavior of Hofbauer cells, the resident macrophages of the placenta. Under normal conditions, these cells maintain an anti-inflammatory phenotype that supports immune tolerance and tissue stability. This state is essential for protecting the fetus, which must coexist with the maternal immune system despite being genetically distinct.
Exposure to particulate pollution alters this balance. Hofbauer cells shift toward a more pro-inflammatory phenotype, characterized by increased expression of activation markers and reduced expression of regulatory markers. Morphologically, these cells appear more activated and exhibit features consistent with increased phagocytic activity.
This transformation closely parallels the behavior of macrophages in inflamed airway tissue. The similarity suggests that macrophage polarization may be regulated at a systemic level, with airway inflammation influencing immune responses across distant epithelial sites, including the placenta.
Developmental Timing and Biological Variability
The effects of environmental exposure are not uniform but depend on the timing of exposure and intrinsic biological factors. Evidence indicates that early gestational exposure, particularly during the first trimester, can disrupt trophoblast differentiation, especially in male fetuses. In contrast, later exposure appears to affect structural and oxygen-delivery components of the placenta more prominently in female fetuses.
These observations highlight the importance of developmental timing and suggest that systemic inflammatory signals intersect with critical windows of cellular differentiation. The result is not simply injury, but altered developmental programming.
From Placental Injury to Clinical Disease
The downstream consequences of these processes are increasingly evident in epidemiological studies. Prenatal exposure to air pollution has been associated with reduced birth weight, as well as increased risks of asthma, allergic diseases, and metabolic dysfunction in childhood.
Within a systems framework, these outcomes can be understood as manifestations of early immune and metabolic programming shaped by systemic inflammation. The placenta serves as both a mediator and a recorder of this process, translating maternal environmental exposures into biological signals that influence fetal development.
This perspective aligns with broader clinical observations that chronic airway inflammation can have far-reaching effects beyond the lungs. Neurocognitive symptoms, cardiovascular dysregulation, and multi-organ epithelial involvement have all been linked to persistent inflammatory states originating in the respiratory system.
Clinical Implications and Future Directions
The recognition of an airway–placenta axis has important implications for clinical practice. It suggests that current approaches to detecting and managing inflammation may be insufficient, particularly when they rely on late-stage markers of disease. Subclinical airway inflammation, which often precedes measurable functional impairment, may play a critical role in shaping systemic outcomes.
Pregnancy may represent a unique window of opportunity for early detection and intervention. Assessing airway inflammation through more sensitive measures could provide insight into systemic inflammatory burden and identify patients at risk for placental dysfunction.
More broadly, this framework calls for a shift toward systems-based thinking in medicine. Conditions traditionally viewed as organ-specific may, in fact, share a common origin in epithelial-driven inflammation that propagates through interconnected biological networks.
Conclusion: A Systems View of Early Life
The emerging evidence supports a fundamental shift in how we understand the relationship between environment and development. The lung functions not only as a site of exposure but as a central regulator of systemic inflammatory tone. The placenta, in turn, responds to and amplifies these signals, shaping the developmental environment of the fetus.
Recognizing this interconnected system reframes prenatal health as part of a broader biological continuum. Environmental exposures, airway inflammation, and immune programming are not isolated events but components of a single, integrated process.
Understanding and intervening in this process may offer new opportunities to improve health not only at birth, but across the lifespan.
Reference
1. Erlandsson L, Hirschmugl B, Hansson E, Mercnik MH, Wadsack C, Hansson SR. Urban air pollution disrupts placental microarchitecture and shifts hofbauer cells towards a pro-inflammatory state. J Environ Sci (China). 2026;160:124-134. doi:10.1016/j.jes.2025.03.043
2. Patlán-Hernández AR, Savouré M, Audureau E, et al. Associations of exposure to outdoor PM2.5 and NO2 during pregnancy with childhood asthma, rhinitis, and eczema in a predominantly rural French mother-child cohort. Environ Pollut. 2024;363(Pt 2):125206. doi:10.1016/j.envpol.2024.125206
3. Saddiki H, Zhang X, Colicino E, et al. DNA methylation profiles reveal sex-specific associations between gestational exposure to ambient air pollution and placenta cell-type composition in the PRISM cohort study. Clin Epigenetics. 2023;15(1):188. Published 2023 Dec 1. doi:10.1186/s13148-023-01601-x
4. Balidemaj F, Flanagan E, Malmqvist E, et al. Prenatal Exposure to Locally Emitted Air Pollutants Is Associated with Birth Weight: An Administrative Cohort Study from Southern Sweden. Toxics. 2022;10(7):366. Published 2022 Jul 1. doi:10.3390/toxics10070366
5. Krempski JW, Dant C, Nadeau KC. The origins of allergy from a systems approach. Ann Allergy Asthma Immunol. 2020;125(5):507-516. doi:10.1016/j.anai.2020.07.013