
Chronic Hives Are More Than a Skin Problem: The Immune Signals Behind Itching, Swelling, and Treatment Response
For someone with chronic spontaneous urticaria, or CSU, the day can begin with clear skin and end with raised, intensely itchy welts covering the arms, legs, or torso. A lip or eyelid may suddenly swell. The rash can disappear within hours, only to emerge somewhere else.
What Happens Beneath a Hive?
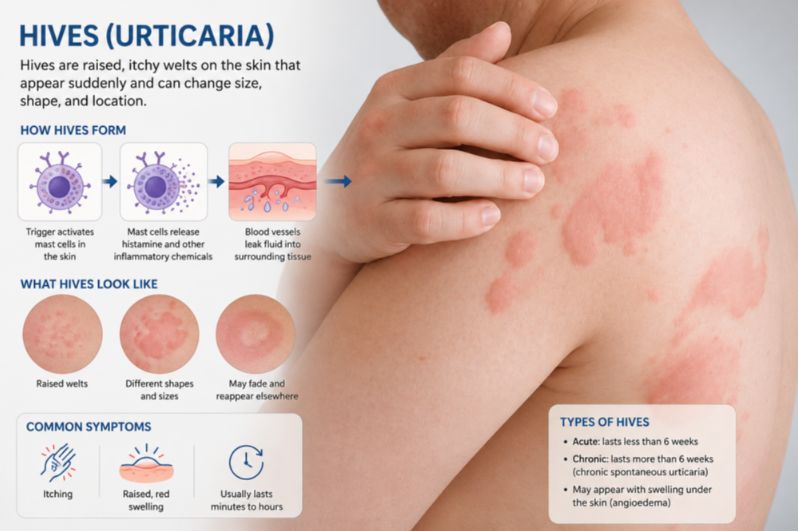
A hive develops when mast cells in the skin release histamine and other inflammatory substances. Small blood vessels dilate and become temporarily leaky, allowing fluid to move into the surrounding tissue. The result is the familiar raised, red or skin-colored wheal.
When this process occurs deeper in the tissue, it can cause angioedema, producing dramatic swelling of the lips, eyelids, hands, feet, or other areas. But what causes mast cells to become repeatedly activated when there is no obvious external trigger?
In some patients, autoantibodies appear to interfere with the IgE–mast cell system. Antibodies directed against IgE or its high-affinity receptor, FcεRI, can potentially activate inflammatory pathways even without conventional exposure to an allergen.
Other patients may have different forms of immune dysregulation. Research into circulating cytokines suggests that several inflammatory pathways can operate simultaneously and may vary considerably from one person to another. This biological diversity may help explain one of the frustrating features of CSU: two people can have nearly identical-looking hives but respond very differently to the same treatment.
IL-31: Connecting the Immune System to the Sensation of Itch
Among the cytokines studied in CSU, IL-31 is particularly interesting because of its close relationship with itching. IL-31 can be produced by immune cells involved in allergic inflammation, including T cells, and has also been linked to mast-cell-associated inflammatory networks. Its receptors are found not only in the skin but also on sensory nerve pathways.
That creates a direct biological bridge between inflammation and sensation. Increased IL-31 activity may therefore help explain why the itch of chronic urticaria can feel disproportionately intense. The sensation is not merely a consequence of damaged or irritated skin. The immune system may be directly communicating with the nervous system.
Research has found higher circulating IL-31 levels in some patients with CSU, particularly among those experiencing severe itching. Interestingly, the intensity of itch does not always perfectly match the overall number or extent of hives. This distinction is important. A patient with fewer visible lesions may still experience severe discomfort if itch-related neuroimmune pathways are highly active.
IL-33: An Alarm Signal From Stressed Tissue
IL-33 belongs to a group of molecules sometimes described as alarmins. These signals are released or become active when tissues are injured, stressed, or disturbed. Once activated, IL-33 can communicate with multiple immune cells and strengthen type 2 inflammatory responses. It can also interact with pathways involved in IgE-dependent mast cell activation.
Studies of IL-33 in CSU have not produced completely uniform results. Differences in patient populations, disease severity, laboratory methods, and timing of blood collection may contribute to apparently conflicting findings.
Even so, some research has associated higher IL-33 concentrations with more severe disease. IL-33 has also been found to correlate with IL-17 and IL-31, raising the possibility that tissue alarm signals, inflammatory T-cell responses, and itch pathways are biologically interconnected. Rather than acting as isolated switches, these cytokines may behave more like members of an inflammatory orchestra, each influencing the activity of the others.
IL-17 and the Inflammatory Side of Chronic Hives
IL-17 is best known for its role in inflammatory and autoimmune diseases. It is strongly associated with a family of immune cells called Th17 cells. Once activated, the IL-17 pathway can promote the production of other inflammatory molecules, including signals connected to TNF-α, IL-1β, and IL-6 pathways. This can create a broader inflammatory environment extending beyond the traditional concept of an IgE-driven allergic reaction.
Some CSU studies have found elevated IL-17 levels, particularly in patients with severe disease. Higher levels have also been associated with increased C-reactive protein, or CRP, a general marker of systemic inflammation, and with lower circulating basophil counts, another laboratory pattern associated with more active CSU in some patients.
These findings support an increasingly important concept: CSU is not necessarily one disease with one immune mechanism. Some patients may have a stronger autoimmune component. Others may show predominantly type 2 inflammation, heightened mast cell activity, Th17-associated inflammation, or a mixture of these processes.
That complexity may eventually become clinically useful. A future blood-based inflammatory profile could potentially help physicians distinguish different CSU subtypes and select therapies more precisely.
Why Omalizumab May Do More Than Block IgE
Omalizumab has transformed the treatment of chronic spontaneous urticaria that remains uncontrolled despite antihistamine therapy.Its best-known action is binding free IgE in the circulation. By reducing the amount of free IgE available to interact with FcεRI receptors, omalizumab gradually reduces the sensitivity of the IgE–mast cell and basophil system.
But newer research suggests that the drug's effects may extend further into the immune network. A 2024 study followed changes in multiple inflammatory cytokines during omalizumab treatment. Over several months, investigators observed changes in cytokines associated with type 2 inflammation.
IL-4 levels increased significantly by the third month of treatment, and this rise was associated with falling disease activity scores. By six months, IL-5 levels had declined significantly, particularly among patients who responded to therapy. IL-17 also tended to decline, especially in patients with severe disease, although the pattern was not uniformly statistically significant across every subgroup.
These findings suggest that successful treatment may involve a gradual reorganization of the inflammatory environment rather than simply an immediate blockade of a single molecule.
Why Some Patients Improve Quickly and Others Take Months
One of the most clinically interesting findings is that the immune system may change differently in early and late responders. Patients who responded early to omalizumab showed an increase in IL-4 by approximately the third month of treatment. Late responders showed a different pattern, including later changes in IL-4 and decreases in IL-5 and IL-33.
Patients who did not respond generally lacked some of the cytokine shifts observed in responders. Higher levels of certain signals, including IL-10 at baseline and IL-13 during treatment, were also explored as possible indicators of treatment resistance.
These findings remain investigational and are not yet ready to serve as routine clinical tests. Cytokine measurements are not currently used in everyday practice to determine whether a patient should continue or stop omalizumab. Still, the research raises an important possibility: a slow clinical response may reflect a different immune trajectory rather than a simple absence of drug effect.
Higher baseline IL-17, for example, has been investigated as a possible marker of delayed response in some patients. If confirmed in larger studies, cytokine profiles might one day help physicians estimate who is likely to respond quickly, who may need more time, and who might benefit from a different biologic strategy.
Could Other Biologic Drugs Treat Chronic Hives?
The expanding cytokine map of CSU has naturally raised interest in treatments targeting immune pathways beyond IgE.IL-4 and IL-13 signaling is one area of particular interest because these cytokines help organize type 2 inflammation. IL-5 is important in eosinophil biology, while IL-17 is involved in a different inflammatory axis associated with Th17 responses.
These biological findings provide a rationale for studying therapies directed at these pathways. However, biological plausibility should not be confused with proven clinical effectiveness. A cytokine can be elevated in a disease without necessarily being the best therapeutic target, and drugs successful in one inflammatory disease do not automatically work in another.
The future of CSU treatment may therefore depend less on finding a single drug for everyone and more on identifying distinct inflammatory subtypes. A patient with predominantly IgE-driven mast cell activation may require a different strategy from someone whose disease has stronger autoimmune or Th17-associated characteristics. Another patient may have overlapping type 2, epithelial alarm, and neuroimmune itch pathways.
The Larger Lesson: Hives Are the Visible End of a Deeper Immune Process
The most important change in our understanding of chronic spontaneous urticaria may be conceptual. The hive is what we see, but it is the final visible product of a much larger biological conversation.
Mast cells release histamine. T cells produce inflammatory cytokines. Damaged or stressed tissues release alarm signals. IgE receptors influence cellular sensitivity. Sensory nerves translate inflammatory messages into itch. These systems communicate continuously, and the balance between them may differ from patient to patient.
This emerging model helps explain why antihistamines work extremely well for some people but incompletely for others. It also helps explain why omalizumab can produce dramatic improvement in one patient within weeks while another requires several months to respond.
Research on IL-17, IL-31, IL-33, and related cytokines is still evolving. The findings are not yet a reason to order broad cytokine panels in routine clinical care, and many observations require confirmation in larger studies. But the direction of the science is becoming clearer: chronic spontaneous urticaria is not merely a superficial rash. It is a complex inflammatory disorder in which allergy-like signaling, autoimmunity, tissue alarm systems, mast cells, and sensory nerves may converge.
Understanding those hidden immune conversations may eventually allow physicians to move beyond treating all chronic hives in the same way, and toward choosing therapy according to the inflammatory biology of each patient.
Reference
1. Lin W, Zhou Q, Liu C, Ying M, Xu S. Increased plasma IL-17, IL-31, and IL-33 levels in chronic spontaneous urticaria. Sci Rep. 2017;7(1):17797. Published 2017 Dec 19. doi:10.1038/s41598-017-18187-z
2. Hoşgören-Tekin S, Eyüboğlu İP, Akkiprik M, Giménez-Arnau AM, Salman A. Inflammatory cytokine levels and changes during omalizumab treatment in chronic spontaneous urticaria. Arch Dermatol Res. 2024;316(6):261. Published 2024 May 25. doi:10.1007/s00403-024-02966-6
3. Nguyen D, Deitiker P. Sustained control of recalcitrant chronic spontaneous urticaria after initiation of inflammatory airway diseases treatment: two case reports. J Med Case Rep. 2024;18(1):113. Published 2024 Feb 23. doi:10.1186/s13256-024-04436-z
4. Dobrican CT, Muntean IA, Pintea I, Petricău C, Deleanu DM, Filip GA. Immunological signature of chronic spontaneous urticaria (Review). Exp Ther Med. 2022;23(6):381. doi:10.3892/etm.2022.11309
5. Kaplan A, Lebwohl M, Giménez-Arnau AM, Hide M, Armstrong AW, Maurer M. Chronic spontaneous urticaria: Focus on pathophysiology to unlock treatment advances. Allergy. 2023;78(2):389-401. doi:10.1111/all.15603