
Depression’s Hidden Fire
Scientists Are Exploring Whether Inflammation May Be Driving Some Forms of Mental Illness
For decades, depression has largely been explained as a disorder of brain chemistry, a problem involving serotonin, dopamine, or stress circuits gone awry. But a growing number of scientists now suspect that, for some patients, depression may also be rooted in something far more physical and ancient: inflammation.
A new clinical trial published in JAMA Psychiatry adds to that provocative idea. Researchers found that blocking a major inflammatory pathway in the immune system produced encouraging improvements in people with difficult-to-treat depression who also showed signs of chronic low-grade inflammation.
The study was small and preliminary. It does not prove that anti-inflammatory drugs can treat depression. Yet it hints at a major shift underway in psychiatry, one that increasingly views at least some mental illnesses not purely as disorders of the mind, but also as disorders of the body.
When the Immune System Affects the Brain
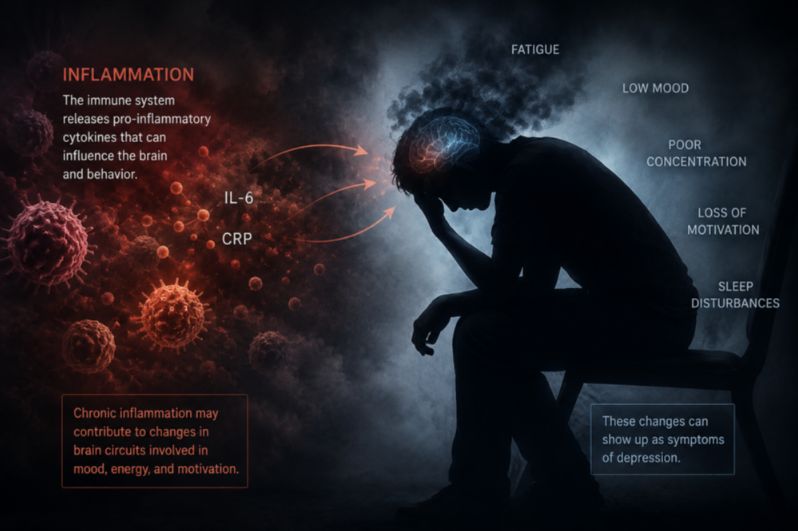
Inflammation is the body’s emergency response system. When we are injured or infected, immune cells release signaling molecules called cytokines that help coordinate defense and repair.
One of those molecules is interleukin-6, or IL-6.In the short term, inflammation is protective. But when the immune system remains chronically activated, as can happen with obesity, chronic stress, autoimmune disease, poor sleep, pollution exposure, or persistent illness, the same inflammatory signals may begin affecting the brain itself.
Scientists have increasingly linked elevated inflammatory markers to symptoms that look remarkably similar to depression: exhaustion, slowed thinking, social withdrawal, poor concentration, disrupted sleep, and loss of motivation.
From an evolutionary perspective, this may not be surprising. During infection, the brain shifts the body into what researchers sometimes call “sickness behavior”, a low-energy state designed to conserve resources while healing. But when inflammation becomes chronic, that biological survival program may become maladaptive. The result may resemble depression.
A Different Kind of Depression
The new study focused on patients whose depression appeared biologically distinct from the classic stereotype of sadness alone.
Researchers recruited adults with moderate-to-severe depression who also had persistent low-grade inflammation, measured using a blood test called high-sensitivity C-reactive protein, or hs-CRP. Participants additionally had prominent physical symptoms such as fatigue, low energy, body heaviness, or slowed functioning. Many had already failed conventional antidepressant therapies.
The investigators randomly assigned participants to receive either a placebo infusion or a single dose of tocilizumab, a medication already used in autoimmune diseases such as rheumatoid arthritis. Tocilizumab works by blocking the IL-6 receptor, effectively dampening part of the inflammatory cascade. Over the following month, a pattern emerged.
Patients receiving the immune-targeting drug experienced higher remission and response rates than those receiving placebo. The differences were especially notable in symptoms tied to energy and physical function, including fatigue, concentration difficulties, agitation, and pessimism.
The benefits also appeared gradual rather than immediate. Improvements became most visible near the end of the four-week study period, suggesting that calming inflammation in the brain may take time to translate into emotional recovery.
Fatigue May Hold the Clues
One of the most intriguing findings involved fatigue.For many patients with depression, fatigue is not merely “feeling tired.” It can feel like moving through wet concrete, an overwhelming physical and cognitive slowing that persists despite sleep, motivation, or willpower.
Traditional antidepressants often struggle to relieve this symptom. In the new study, however, fatigue showed some of the strongest signals of improvement after inflammatory blockade. That finding aligns with a growing theory that inflammatory depression may disproportionately affect brain systems involved in energy regulation, motivation, reward processing, and physical drive.
In other words, some depressed patients may not primarily suffer from a deficit of happiness. Instead, they may be experiencing a brain trapped in a prolonged biological “illness mode.”
The Blood Test That Could Change Psychiatry
Perhaps the study’s most important discovery was not the medication itself, but who appeared most likely to benefit from it. Researchers found that higher baseline hs-CRP levels predicted greater antidepressant effects from IL-6 blockade. The more inflammation patients had at the start, the stronger the treatment signal appeared to become.
Curiously, IL-6 blood levels themselves did not predict response. That distinction matters because hs-CRP is already a routine and inexpensive laboratory test widely used in cardiovascular medicine. If future trials confirm the findings, psychiatry could someday begin using inflammatory biomarkers to guide treatment decisions.
Such an approach would represent a profound change in the field. For much of modern psychiatry, diagnoses have been based primarily on symptom checklists rather than biological measurements. But the emerging science of “precision psychiatry” aims to identify biologically distinct subtypes of depression that may respond to different therapies.Inflammation may become one of those biological fingerprints.
Depression Beyond Brain Chemistry
The findings also challenge a long-standing cultural divide between “mental” and “physical” illness.Inflammation does not recognize that distinction.
Immune molecules can influence neurotransmitters, stress hormones, sleep cycles, metabolism, and neural connectivity. Chronic inflammation has already been linked to cardiovascular disease, diabetes, autoimmune disorders, neurodegeneration, and now increasingly, psychiatric disease.
Some researchers believe depression should no longer be viewed as a single disorder at all. Instead, it may represent many overlapping conditions that share outward emotional symptoms but arise from different biological drivers.
For one patient, trauma may dominate. For another, genetics or circadian disruption. For another, chronic immune activation.All may carry the same diagnosis while requiring very different treatments.
A Promising but Early Frontier
The researchers caution that the study remains a proof-of-concept trial, not a definitive demonstration of effectiveness. Only 30 participants were enrolled, and larger studies are essential before immune therapies could become part of mainstream psychiatric care.
There are also important practical concerns. Drugs that suppress immune signaling can increase infection risks and are far more complex than standard antidepressants. The goal is unlikely to be giving powerful immune medications to every depressed patient. Instead, scientists are searching for a narrower group: patients whose depression appears biologically tied to chronic inflammation.
Still, the implications are difficult to ignore.If future research confirms that immune dysfunction can directly contribute to depression, psychiatry may eventually move closer to the rest of medicine, using laboratory markers, biological pathways, and targeted therapies to tailor treatment to the individual patient.
The mind, after all, has never been separate from the body. The immune system may simply be one more bridge connecting the two.
Reference
1. Foley ÉM, Turner N, Margelyte R, et al. Interleukin 6 as a Treatment Target for Depression: A Proof-of-Concept Randomized Clinical Trial. JAMA Psychiatry. Published online May 20, 2026. doi:10.1001/jamapsychiatry.2026.1053
2. Miller AH, Raison CL. The role of inflammation in depression: from evolutionary imperative to modern treatment target. Nat Rev Immunol. 2016;16(1):22-34. doi:10.1038/nri.2015.5
3. Dantzer R, O'Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008;9(1):46-56. doi:10.1038/nrn2297
4. Raison CL, Rutherford RE, Woolwine BJ, et al. A randomized controlled trial of the tumor necrosis factor antagonist infliximab for treatment-resistant depression: the role of baseline inflammatory biomarkers. JAMA Psychiatry. 2013;70(1):31-41. doi:10.1001/2013.jamapsychiatry.4
5. Osimo EF, Baxter LJ, Lewis G, Jones PB, Khandaker GM. Prevalence of low-grade inflammation in depression: a systematic review and meta-analysis of CRP levels. Psychol Med. 2019;49(12):1958-1970. doi:10.1017/S0033291719001454