
Caffeine, Cigarettes, and a President: The Wild History of Asthma Before Inhalers
The Disease That Medicine Could Hear but Not Explain
Asthma in the 1800s: A Mystery of “Fits” and Suffocation
By the early 19th century, asthma was already a familiar disease, although physicians understood almost nothing about its biological mechanisms. Doctors described “fits” of breathlessness accompanied by wheezing and chest tightness. The disease appeared episodic and mysterious. A patient could seem healthy during the day and nearly suffocate hours later.
Without X-rays, pulmonary function testing or modern immunology, physicians relied largely on observation. The newly invented stethoscope allowed them to hear wheezing within the chest, but diagnosis still depended mostly on listening to patient stories and excluding deadlier illnesses such as tuberculosis or heart failure.
Treatment often bordered on the improvised. Patients inhaled steam. Some smoked preparations made from Datura stramonium, also known as thorn-apple, whose naturally occurring anticholinergic compounds could transiently relax airway muscles. Others inhaled the fumes of various herbal mixtures, many of which were ineffective or dangerous. Yet in retrospect, these crude remedies hinted at something medicine would later confirm: asthma involved reversible airway narrowing.
Theodore Roosevelt’s Childhood Battle for Air
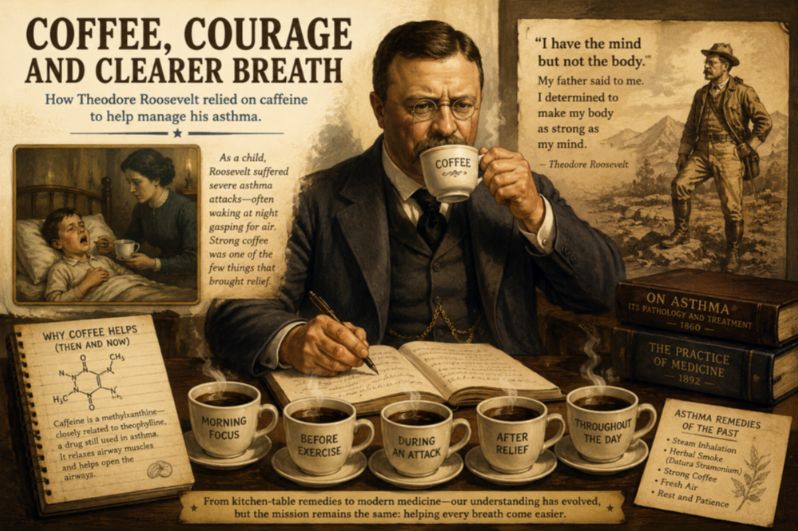
In Roosevelt’s childhood during the mid-1800s, severe asthma could feel like a family emergency without a solution. Historical accounts describe the young Roosevelt gasping desperately for air while relatives carried him outside into cold nighttime streets or drove him rapidly through New York in horse-drawn carriages because moving air sometimes provided relief. The attacks were terrifying not only because they impaired breathing, but because no one fully understood why they occurred.
His father responded with a philosophy that would shape Roosevelt’s life. If his son possessed a strong mind trapped in a weak body, then the body, he believed, must be trained. Roosevelt embraced exercise, outdoor exposure and physical exertion with almost obsessive determination. The irony, of course, is that vigorous exercise can itself trigger asthma symptoms. Yet for Roosevelt, physical training became both therapy and identity.
Over time, the frail child who once struggled through sleepless nights transformed himself into one of the most physically energetic political figures in American history. But asthma never entirely disappeared from his life. Rather, it became something he constantly battled against.
When Coffee Was Considered Asthma Medicine
At the same time, another asthma treatment quietly became woven into daily life: coffee.
Today caffeine is discussed mainly in terms of productivity, sleep deprivation or cardiovascular health. In the 19th and early 20th centuries, however, strong black coffee was widely recognized as an asthma remedy. Physicians recommended it because patients often noticed that it eased breathing during attacks.
Modern pharmacology explains why.
Caffeine belongs to a chemical class called methylxanthines, closely related to theophylline, one of the major asthma medications used throughout much of the 20th century. Both compounds relax airway smooth muscle and stimulate respiration. Before inhalers existed, a strong cup of coffee could function as a rudimentary bronchodilator.
The doses could be extraordinary. Historical reports describe patients consuming multiple cups of intensely brewed coffee in rapid succession during asthma attacks. The resulting tremors, palpitations and insomnia were considered acceptable tradeoffs compared with the terror of suffocation.
In some ways, this represented one of medicine’s earliest examples of translational physiology. Patients recognized empirically that caffeine improved breathing long before scientists understood the molecular pathways involved. The transition from coffee to pharmaceutical theophylline would later formalize that observation into modern respiratory medicine.
The Era of Adrenaline, Ephedrine and “Asthma Cigarettes”
By the 1920s, asthma care entered a transitional scientific age. Physicians began identifying allergic triggers such as ragweed and animal dander. Blood eosinophils emerged as biological clues to the disease. Skin testing allowed clinicians to classify some patients as having “extrinsic asthma,” an early recognition that environmental hypersensitivity played a role.
Treatment also became more aggressive. Adrenaline injections rapidly relieved airway constriction and became standard emergency therapy. Ephedrine, derived from traditional Chinese medicine, provided longer-lasting bronchodilation. Meanwhile “asthma cigarettes,” containing compounds such as belladonna and stramonium, remained commercially popular well into the early 20th century.
The image now feels paradoxical: physicians prescribing smoke inhalation for respiratory disease. Yet it reflected the fragmented understanding of the era. Doctors knew airway muscles could constrict and relax, but they had not yet grasped the chronic inflammatory biology beneath the disease.
The Modern Revolution in Asthma Care
The modern asthma era emerged only after mid-century, when spirometry transformed breathing into something measurable. Physicians could now quantify airflow obstruction and demonstrate its reversibility after bronchodilator therapy. Researchers increasingly recognized asthma not simply as intermittent bronchospasm, but as chronic airway inflammation. Inhaled corticosteroids shifted treatment away from crisis management and toward long-term inflammatory control.
Today biologic therapies can target specific immune pathways involving IgE, eosinophils and cytokines with remarkable precision. A disease once treated with smoke and coffee can now be managed with monoclonal antibodies engineered at the molecular level.
What Has, and Has Not, Changed
And yet asthma remains strangely unchanged.
The wheezing described by physicians in 1828 would sound familiar in any emergency department today. Patients still wake at night gasping for breath. Children still sit upright during attacks because lying flat worsens the sensation of suffocation. The emotional experience of asthma, the panic, chest tightness and primal fear associated with not getting enough air, has remained constant across centuries.
What changed was humanity’s ability to intervene before the crisis became catastrophic.
That may be the deeper lesson hidden within Roosevelt’s story. Modern audiences often interpret his life as a triumph of determination over physical weakness. But his childhood also serves as a reminder of how recently asthma transformed from a largely uncontrollable condition into a medically manageable one.
Before inhalers, survival often depended on environmental luck, family vigilance, physical adaptation and stimulants brewed in kitchen pots. In that world, coffee was not merely comfort. For many patients, it was medicine.
Reference
1. von Mutius E, Drazen JM. A patient with asthma seeks medical advice in 1828, 1928, and 2012. N Engl J Med. 2012;366(9):827-834. doi:10.1056/NEJMra1102783
2. Theodore Roosevelt. An Autobiography. New York, NY: Macmillan; 1913.
3. Barnes PJ. Theophylline. Am J Respir Crit Care Med. 2013;188(8):901-906. doi:10.1164/rccm.201302-0388PP
4. Henry Hyde Salter. On Asthma: Its Pathology and Treatment. London, UK: John Churchill & Sons; 1860.
5. Holgate ST. Pathogenesis of asthma. Clin Exp Allergy. 2008;38(6):872-897. doi:10.1111/j.1365-2222.2008.02971.x